

Testicular cancer starts in the male gland known as a testicle or testis (two are called testicles, or testes). Though it can affect a man or boy at any age, it is most often found in men age 15 to 44 years. It’s fairly rare and very treatable. With early diagnosis, testicular cancer can be cured. With treatment, the risk of death from this cancer is small.
How well a patient reacts to treatment depends on the cancer cell-type, whether it has spread and the patient’s overall health. Doctors treating testicular cancer will aim to limit treatment side effects.
To catch this cancer early, men are encouraged to learn about early signs, learn how to do a testicular self-exam and talk with a health care provider if there is a suspicious lump, swelling, or pain in the area.
The Testicles
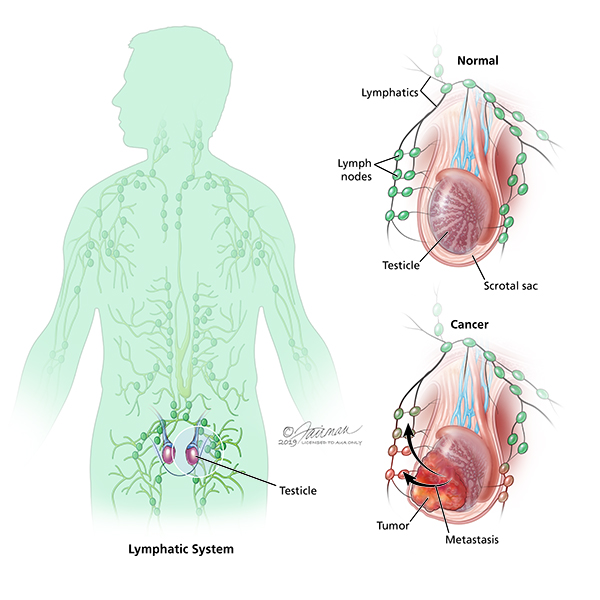
The testicles are part of the male reproductive system. These two small egg-shaped glands are held in a sac (scrotum) below the penis.
The testicles have a firm, slightly spongy feel. The firmness of the testicle should be the same throughout. The size of the testicles should also be about the same, though one may be larger than the other. At the top and outside edge is a rubbery, tube-like structure called the epididymis.
The testicles are where sperm mature. The testicles also make male hormones such as testosterone. This hormone controls the sex drive in men. It also starts the growth of muscle, bone and body hair.
Symptoms
Signs of a testicular tumor are:
- A painless lump in the testicle (the most common sign)
- Swelling of the testicle (with or without pain) or a feeling of weight in the scrotum
- Pain or a dull ache in the testicle, scrotum or groin
- Tenderness or changes in the male breast tissue
If you find any lump or firm part of the testicle, you should see a doctor to find out if it is a tumor. Very few men who have testicular cancer felt pain at first.
Many men do not tell their health care provider about these signs. On average, men wait for about five months before saying anything. Since the tumor can spread during that time, it is vital to reach out to a urologist if you notice any of these signs. This is especially true if a sign lasts for more than two weeks. The urologist will want to test if cancer is growing or if there’s some other issue, like:
- Epididymitis: swelling of the epididymis. Often treated with antibiotics.
- Testicular torsion: twisting of the testicles. Often treated with surgery.
- Inguinal hernia: when part of the intestine pokes through a weak part of the stomach muscles near the groin. Often treated with surgery.
- Hydrocele: when fluid builds up in the scrotum. This often goes away without treatment.
Diagnosing Testicular Cancer
The Testicular Self-Exam
The best time to do a testicular self-exam is after a warm bath or shower, while standing, when the scrotum is relaxed. It only takes a few minutes. To start:
- Check each testicle. Gently but firmly roll each testicle between the thumb and forefingers. Feel the whole surface. The firmness of the testis should be the same all around. It’s normal for one testis to be slightly larger than the other.
- Find the epididymis and vas deferens. These are soft, tube-like structures above and behind the testicle. These tubes collect and carry sperm. Just become familiar with how these cords feel.
- Look for lumps, swelling or things that don’t seem right. Lumps or bumps are not normal (even if they cause no pain). Pain is not normal.
- Check yourself at least once per month. Always look for any changes in size, shape, or texture.
If you notice a lump or any changes over time, you should seek medical help. It may be nothing, but if it is testicular cancer, it can spread very quickly. When found early, testicular cancer is very curable. If you have any questions or concerns, talk to your urologist.
Medical Exam
- Health record and physical exam: Your urologist will talk with you about your health. They will examine your scrotum, belly (abdomen), lymph nodes, and other parts to look for signs of cancer. They will look for lumps, firmness or signs of swelling. Tell them if you have a history of undescended testes.
- Testicular ultrasound: This imaging test is used to see inside the scrotum and to check a suspicious lump. Other scans or x-rays may be done if your doctor would like to see inside your chest or abdomen. This is done to see if cancer has spread to lymph nodes, the lungs or liver. MRIs are rarely used, but needed in some cases to check the brain and spinal cord.
- Blood test: A blood test is taken to check tumor markers. These are proteins and hormones made by some testicular cancers. AFP, ACG and LDH tumor markers rise with some cancers but many testicular cancers will not produce tumor markers. In other words, just because tumor markers are normal does not mean that you are free of cancer. It’s of great value to ask your doctor about your tumor maker levels and learn what’s normal vs. not normal.
- Serum Tumor Marker Test: Tumor markers (AFP, HCG, and LDH) should be measured before any treatment, such as surgery. If cancer is found, tumor marker tests will be repeated after treatment to track how well you’re doing over time. Some medicines and marijuana can create false positive levels of HCG. Tell your doctor about your medicine and/or marijuana use.
- Pure seminomas can raise HCG levels but never AFP levels.
- Non-seminomas often raise AFP and/or HCG levels.
- Serum Tumor Marker Test: Tumor markers (AFP, HCG, and LDH) should be measured before any treatment, such as surgery. If cancer is found, tumor marker tests will be repeated after treatment to track how well you’re doing over time. Some medicines and marijuana can create false positive levels of HCG. Tell your doctor about your medicine and/or marijuana use.
Stages of Testicular Cancer
If your urologist finds cancer through these exams, he or she will want to learn the exact cancer cell-type and if it has spread. This is called “staging.” This process helps the doctor learn which treatments are best.
Unlike other cancers, your doctor does not take a tissue sample (biopsy) before surgery. With testicular cancer, cells are looked at after surgery is done to remove the cancerous tissue.
Stages
- Stage 0: This is also called “Germ Cell Neoplasia In Situ (GCNIS)”. This is not really cancer, but a warning that cancer could grow. GCNIS may be found in the seminal tubules and nowhere else.
- Stage I (IA, IB, IS): Cancer is found only in the testicle. It has not spread to nearby lymph nodes.
- Stage II (IIA, IIB, IIC): Cancer has spread to one or more lymph nodes in the abdomen (belly). It has not spread to other parts of the body.
- Stage III (IIIA, IIIB, IIIC): Cancer has spread beyond the lymph nodes in the abdomen. Cancer may be found far from the testicles, like in distant lymph nodes or the lungs. Tumor marker levels are high.
More than 90% of testicular cancers start in cells known as germ cells. These are the cells that make sperm. The main types of germ cell tumors (GCTs) in the testicles are either seminomas or non-seminomas:
- Seminoma – The most common cell type of testicular cancer. They grow slowly and react well to chemotherapy and radiation. Pure seminomas can raise HCG levels but never AFP levels. In addition to surgery, this type of cancer reacts well to radiation and chemotherapy treatment. Active surveillance (monitoring) is often used for low-stage seminomas.
- Non-seminomas – There are a few types of non-seminomas: choriocarcinoma, embryonal carcinoma, teratoma and yolk sac tumors. These cells grow more quickly and are less responsive to radiation and chemotherapy. Non-seminomas often raise AFP and/or HCG levels. Treatment for this type of cancer can involve surveillance and surgery. Later stages may be treated with chemotherapy. Sometimes more surgery is needed.
There are also rare testicular cancers from cells that support other roles. Leydig cell tumors form from the Leydig cells that make testosterone. Sertoli cell tumors come from the Sertoli cells that support normal sperm growth.
Testicular cancer may involve more than one cell-type. The best treatment will depend on the diagnosis (such as stage and risk of the cancer coming back after treatment) and whether the disease has spread.
Treatments
Often, a team of doctors (urologist, oncologist, radiation oncologist) will work together to find the best treatment plan for each patient. Choices will be based on the exact diagnosis and health of the patient. Treatment options include:
- Surveillance
- Surgery
- Radiation
- Chemotherapy
Before any treatment starts, men should talk with their urologist about if they want to have a child. Infertility and changes in male hormones are common after certain treatments. Sperm banking may be useful before treatment, mostly if you hope to have children in the future.
Men can also ask about a testicular prosthesis (fake body part) before surgery. This is a way to make the testicles look more “normal” after a testis is removed.
Surveillance
Surveillance is a way to look for changes with normal check-ups. These include a physical exam, tumor marker tests, and imaging tests. Imaging tests start with an ultrasound of the scrotum. They can also involve chest x-rays or CT scans. No matter what treatment, most men should be checked for signs of low-testosterone as well.
Surveillance is recommended for Stage 0 and some Stage 1 cancers.
- Patients with stage I seminoma. It should involve a physical exam, tumor marker test and imaging:
- Every 4-6 months for the first 2 years; every 6-12 months in years 3-5
- Patients with stage 1 non-seminoma germ cell tumors (NSGCT), after surgery. It should include a physical exam and tumor marker test:
- Every 2-3 months in year 1; every 2-4 months in year 2; every 4-6 months in year 3; every 6-12 months in years 4-5
- Patients with stage I NSGCT, after surgery. It should involve a chest x-ray and other imaging:
- Every 4-6 months in year 1; every 4-12 months in year 2; one time in years 3-5
If the cancer shows signs of growth, or if hormone levels change, then more treatment may be offered. If not, only surveillance is needed.
Surgery
Surgery is the main treatment for testicular cancer. Most often, an orchiectomy is done to remove the entire testis. Depending on the diagnosis, other options may be offered. Changes in fertility should be discussed first.
- Orchiectomy is used to diagnose and treat both early-stage and later-stage testicular cancer. This surgery removes the entire testicle and mass through a small cut in the groin. The spermatic cord is also removed. The cell type will be confirmed and staged with this surgery.
- After surgery, regular surveillance is done to make sure the cancer doesn’t return.
- If one testicle is removed and the other is normal, testosterone levels should be fine. The remaining, healthy testicle should make enough testosterone. (10-15% of testicular cancer survivors will have low testosterone levels and can get treatment.)
- If a man is concerned about the way he looks, a testicular prosthesis is an option.
- Testis-sparing surgery (TSS) is only recommended in select cases. This surgery removes just the tumor tissue, not the entire testis. For this, the mass must be very small and tumor markers must be negative. This is best for men with benign tumors, rather than cancer.
- When TSS is done, regular surveillance is important because the cancer can return. Other side effects, like infertility, are possible.
- If the tumor is malignant, and the man has a normal testicle on the other side, then TSS is not recommended.
- Retroperitoneal lymph node dissection (RPLND) is a complex surgery used to limit the side effects of removing the lymph nodes in the back of the abdomen. A skilled surgeon is used and it can be helpful for some men. This surgery is an option for patients with stage I cancer and a high risk for recurrence. It is typically for men with non-seminomatous germ cell tumors. It can be used rather than chemotherapy for patients with stage IIA or IIB non-seminoma tumors.
- After RPLND surgery, chemotherapy or surveillance is offered depending on the cancer location, type and risk of recurrence.
- It is important to work with a highly experienced surgeon.
Radiation
Radiation is used to kill cancer cells on the testis or in nearby lymph nodes. It is used for seminoma-cell cancers, because some forms of non-seminoma are resistant to radiation. It may be an option if testicular cancer (either type) has spread to distant organs like the brain. There are a few radiation therapy types used.
Chemotherapy
Chemotherapy is used for cancers that spread beyond the testicles, or if tumor markers rise after surgery. Serum tumor markers and imaging tests help guide how much chemotherapy to use, and if it can help.
These drugs travel through the body in the bloodstream and cause side effects. They can wipe out cancer cells that may have traveled to lymph nodes. It’s also used to help lower the risk of cancer coming back after surgery.
Sometimes, more than one chemotherapy drug may be combined for testicular cancer treatment. These drugs are given in three or four, three-week cycles. Sometimes more surgery will be done to remove tumors after chemo.
Further Treatment
Beyond basic surgery, care depends on the type of cancer cell and results. Even if cancer was found early and treated, follow-up tests are recommended.
If, after time, cancer returns, then more treatment will be needed.
Incidence and Statistics (US)
Rate of New Cases and Deaths per 100,000: The rate of new cases of testicular cancer was 5.9 per 100,000 men per year. The death rate was 0.3 per 100,000 men per year. These rates are age-adjusted and based on 2013–2017 cases and deaths.
Lifetime Risk of Developing Cancer: Approximately 0.4 percent of men will be diagnosed with testicular cancer at some point during their lifetime, based on 2015–2017 data.
Prevalence of This Cancer: In 2017, there were an estimated 269,769 men living with testicular cancer in the United States.

{kind=link}