Testicular cancer starts in the male gland known as a testicle or testis (two are called testicles, or testes). Though it can affect a man or boy at any age, it is most often found in men age 15 to 44 years. It’s fairly rare and very treatable. With early diagnosis, testicular cancer can be cured. With treatment, the risk of death from this cancer is small.
How well a patient reacts to treatment depends on the cancer cell-type, whether it has spread and the patient’s overall health. Doctors treating testicular cancer will aim to limit treatment side effects.
To catch this cancer early, men are encouraged to learn about early signs, learn how to do a testicular self-exam and talk with a health care provider if there is a suspicious lump, swelling, or pain in the area.
The testicles are part of the male reproductive system. These two small egg-shaped glands are held in a sac (scrotum) below the penis.
The testicles have a firm, slightly spongy feel. The firmness of the testicle should be the same throughout. The size of the testicles should also be about the same, though one may be larger than the other. At the top and outside edge is a rubbery, tube-like structure called the epididymis.
The testicles are where sperm mature. The testicles also make male hormones such as testosterone. This hormone controls the sex drive in men. It also starts the growth of muscle, bone and body hair.
Signs of a testicular tumor are:
If you find any lump or firm part of the testicle, you should see a doctor to find out if it is a tumor. Very few men who have testicular cancer felt pain at first.
Many men do not tell their health care provider about these signs. On average, men wait for about five months before saying anything. Since the tumor can spread during that time, it is vital to reach out to a urologist if you notice any of these signs. This is especially true if a sign lasts for more than two weeks. The urologist will want to test if cancer is growing or if there’s some other issue, like:
The best time to do a testicular self-exam is after a warm bath or shower, while standing, when the scrotum is relaxed. It only takes a few minutes. To start:
If you notice a lump or any changes over time, you should seek medical help. It may be nothing, but if it is testicular cancer, it can spread very quickly. When found early, testicular cancer is very curable. If you have any questions or concerns, talk to your urologist.
If your urologist finds cancer through these exams, he or she will want to learn the exact cancer cell-type and if it has spread. This is called “staging.” This process helps the doctor learn which treatments are best.
Unlike other cancers, your doctor does not take a tissue sample (biopsy) before surgery. With testicular cancer, cells are looked at after surgery is done to remove the cancerous tissue.
More than 90% of testicular cancers start in cells known as germ cells. These are the cells that make sperm. The main types of germ cell tumors (GCTs) in the testicles are either seminomas or non-seminomas:
There are also rare testicular cancers from cells that support other roles. Leydig cell tumors form from the Leydig cells that make testosterone. Sertoli cell tumors come from the Sertoli cells that support normal sperm growth.
Testicular cancer may involve more than one cell-type. The best treatment will depend on the diagnosis (such as stage and risk of the cancer coming back after treatment) and whether the disease has spread.
Often, a team of doctors (urologist, oncologist, radiation oncologist) will work together to find the best treatment plan for each patient. Choices will be based on the exact diagnosis and health of the patient. Treatment options include:
Before any treatment starts, men should talk with their urologist about if they want to have a child. Infertility and changes in male hormones are common after certain treatments. Sperm banking may be useful before treatment, mostly if you hope to have children in the future.
Men can also ask about a testicular prosthesis (fake body part) before surgery. This is a way to make the testicles look more “normal” after a testis is removed.
Surveillance is a way to look for changes with normal check-ups. These include a physical exam, tumor marker tests, and imaging tests. Imaging tests start with an ultrasound of the scrotum. They can also involve chest x-rays or CT scans. No matter what treatment, most men should be checked for signs of low-testosterone as well.
Surveillance is recommended for Stage 0 and some Stage 1 cancers.
If the cancer shows signs of growth, or if hormone levels change, then more treatment may be offered. If not, only surveillance is needed.
Surgery is the main treatment for testicular cancer. Most often, an orchiectomy is done to remove the entire testis. Depending on the diagnosis, other options may be offered. Changes in fertility should be discussed first.
Radiation is used to kill cancer cells on the testis or in nearby lymph nodes. It is used for seminoma-cell cancers, because some forms of non-seminoma are resistant to radiation. It may be an option if testicular cancer (either type) has spread to distant organs like the brain. There are a few radiation therapy types used.
Chemotherapy is used for cancers that spread beyond the testicles, or if tumor markers rise after surgery. Serum tumor markers and imaging tests help guide how much chemotherapy to use, and if it can help.
These drugs travel through the body in the bloodstream and cause side effects. They can wipe out cancer cells that may have traveled to lymph nodes. It’s also used to help lower the risk of cancer coming back after surgery.
Sometimes, more than one chemotherapy drug may be combined for testicular cancer treatment. These drugs are given in three or four, three-week cycles. Sometimes more surgery will be done to remove tumors after chemo.
Beyond basic surgery, care depends on the type of cancer cell and results. Even if cancer was found early and treated, follow-up tests are recommended.
If, after time, cancer returns, then more treatment will be needed.
Rate of New Cases and Deaths per 100,000: The rate of new cases of testicular cancer was 5.9 per 100,000 men per year. The death rate was 0.3 per 100,000 men per year. These rates are age-adjusted and based on 2013–2017 cases and deaths.
Lifetime Risk of Developing Cancer: Approximately 0.4 percent of men will be diagnosed with testicular cancer at some point during their lifetime, based on 2015–2017 data.
Prevalence of This Cancer: In 2017, there were an estimated 269,769 men living with testicular cancer in the United States.
In the health system, news coverage naturally gravitates toward breakthroughs. A new therapy, a diagnostic…
I first learned about the urban heat island effect in a high school geography class.…
Artificial intelligence is advancing in health care faster than almost any other technology in modern…
Throughout the history of science, it has rarely been the case that any phenomenon has…
Mandates and strong recommendations have been the key to successful vaccination programmes protecting people for…
Brain organoids, sometimes called “mini-brains,” are three-dimensional clusters of human brain cells grown in labs from pluripotent stem…
This website uses cookies. Your continued use of the site is subject to the acceptance of these cookies. Please refer to our Privacy Policy for more information.
Read More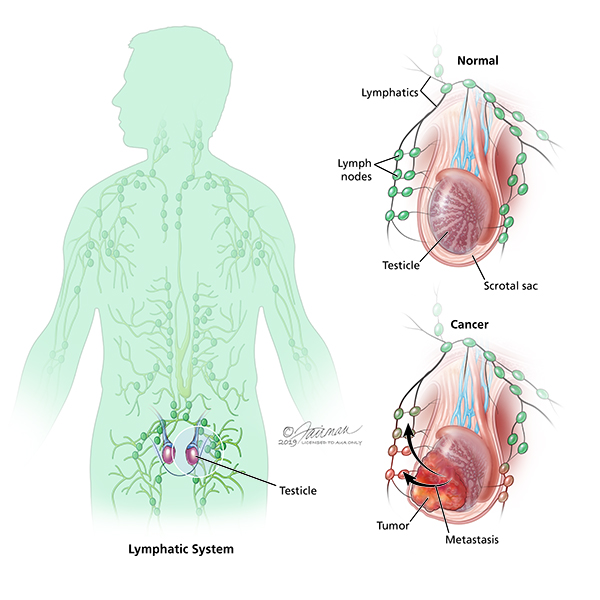{kind=link}